
What is the Glucose Management Indicator (GMI)?
With more people using continuous glucose monitoring to measure their blood glucose levels, a new metric known as the glucose management indicator (GMI) has been developed to help health professionals, and people living with diabetes, to gain greater insight into blood glucose fluctuations. Carolien Koreneff, an experienced credentialled diabetes educator and registered nurse, explains what GMI is, how it is measured, and how to interpret results.
Glucose levels
Both blood glucose and sensor glucose monitoring give the user a number as an indication of how much glucose is in the body. However, it is important to note that finger prick blood glucose monitors and flash or continuous glucose monitors measure glucose from different sources. Finger prick blood glucose monitors measure glucose in the blood, whereas flash and continuous glucose monitors measure the glucose in the interstitial fluid. Hence the numbers from these two systems, even if taken at the same time, will rarely be the same.
If a venous sample was taken at the same time as the blood glucose or sensor glucose level, the laboratory result will give a third number. To date, this lab result is considered the most accurate number. There is no direct comparison between the blood glucose (BG) and sensor glucose (SG) reading. Each will be compared to the lab results, not to each other.
There are many factors that contribute to a difference between the BG and SG readings. Unwashed hands are the most common reason for inaccurate blood glucose readings. Users of blood glucose monitors should always clean their hands with soap and water to remove any sugar from their fingers, and it is also vital that they dry their hands thoroughly. Wiping away the first drop of blood with a clean tissue or a gauze is a great way to further improve accuracy.
It is also crucial that blood glucose monitoring strips remain stored in their original packaging, are used within three months of opening the packaging, and that they have not past the expiration date.
Newly inserted sensors may show a greater discrepancy between the SG and BG on day one. However, generally the numbers get closer over the first 24 hours.
HbA1c
In the article HbA1c Overview for Health Professionals we explained that a HbA1c, or glycated haemoglobin, blood test highlights long-term blood glucose levels. It does this by measuring how much glucose is attached (glycated) to the haemoglobin (Hb) in the blood stream. Haemoglobin is the protein in the red blood cells that also carries oxygen throughout the body.
As Hb generally lives for around 120 days, the HbA1c gives an average of how much glucose has been in the blood over the past few months. However, HbA1c is a weighted average of glucose levels, this means that glucose levels in the past 30 days contribute substantially more to the level of HbA1c, than do glucose levels from 90-120 days earlier.
HbA1c is an important marker for overall glycaemic management, and it is also a significant risk indicator for diabetes complications. However, HbA1c used alone does not highlight the presence of clinically important glucose variability. Nor does it show the timing and the extent of any hypo- or hyperglycaemia. Hence HbA1c may be insufficient to optimally guide a personalised therapy change, particularly in people with diabetes taking insulin.
eA1c
Estimated A1c (eA1c) is the old measure used to convert the mean glucose obtained from CGM or self-monitored blood glucose readings.
Ten days of CGM data is generally enough to estimate the average glucose, time-in-target range, and time-in-hyperglycaemia. CGM data collected over 14 days or more offers a better estimate for time-in-hypoglycaemia, and of glucose variability. Hence, CGM data collected for at least 10–14 days gives enough information to create a representative CGM-derived mean glucose value.
From this mean glucose value, and using a standard formula, the eA1C could be generated. This was intended to be equivalent to the value of a HbA1c level measured simultaneously in a laboratory.
Many health professionals used the eA1C as an educational tool, but some found it confusing or got frustrated if the eA1C and laboratory-measured HbA1c did not match. For some people the eA1c was very similar to the laboratory measured HbA1c, but for others it was higher or lower than the actual HbA1c. To avoid any further confusion, the Food and Drug Administration (FDA) in the USA decided that, the terminology of eA1C needed to change.
Glucose Management Indicator (GMI)
Researchers worked toward a solution, which included renaming the eA1C to the glucose management indicator (GMI). This name was chosen, after consultation with health professionals, people living with diabetes, diabetes advocacy organisations and manufacturers of glucose monitoring systems, as it conveys that this is a measure derived from glucose values and can provide an indication of the current state of a person’s glucose management.
They created a new formula, using the most accurate CGM systems available and based on recent clinical trials, for converting CGM-derived mean glucose to GMI. They also provided new CGM analyses and explanations to further understand how to interpret GMI, and use it most effectively in clinical practice.
GMI is calculated using a formula based on a graph that compares CGM-measured mean glucose concentration (shown on the horizontal x-axis) with central laboratory-measured HbA1c values (shown on the vertical y-axis).
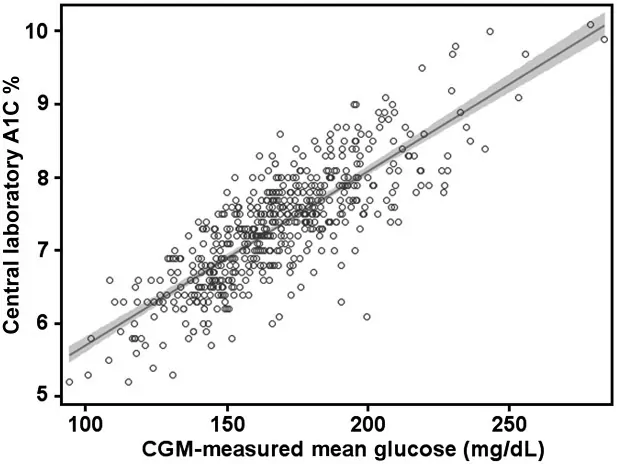
Image from https://pmc.ncbi.nlm.nih.gov/articles/PMC6196826/ © 2018 by the American Diabetes Association.
The shaded area, in the table above, represents the 95% confidence interval (CI) of the regression line.
To calculate GMI you can use this formula:
GMI (%) = 3.31 + 0.02392 × [average glucose in mg/dL].
If you are using average glucose measured in mmol/L and the International Federation of Clinical Chemistry (IFCC) standards for A1C, the formula is:
GMI (mmol/mol) = 12.71 + 4.70587 × [average glucose in mmol/L].
GMI calculators are available at www.jaeb.org/gmi and www.AGPreport.org/agp/links.
Please note at least 10, and preferably 14 or more, days of CGM should be used when calculating GMI. It is also important to note that, since all four studies used to derive the above formulas used Dexcom sensors, we currently can’t be sure the formula will be exactly the same for data from other manufacturer’s sensors. However, the formula is likely to be similar, provided the other sensors are fairly accurate and aren’t consistently off in one particular direction.
What if GMI and HbA1c are different?
There can be a difference between GMI and HbA1c, for example during periods of acute hyperglycaemia, such as during illness or steroid treatment. In this case the GMI is likely to be higher than the HbA1c.
The opposite also can occur, where the GMI is lower than the laboratory HbA1c. This can happen during periods of much lower-than-usual glucose readings (for example, when starting a lower carbohydrate diet, an intensive exercise regimen, or during the first few weeks after starting a new, effective glucose-lowering medication).
Most of the time, when there are no acute or dramatic changes from a person’s usual glucose levels, the difference between GMI and A1C can help inform diabetes management and help set personalised diabetes management goals.
If a person has a GMI always considerably lower than expected from a measured HbA1c, for example, if the target HbA1c is 7.0% but the GMI is always lower (say 6.6%), make sure that the time spent in hypoglycaemia (Time Below Range, or TBR) is not excessive.
If a person has a GMI always considerably higher than expected from a measured A1C, for example if the target A1C is 7.5% and the GMI is always higher (say 7.9%), it might be safe to set the HbA1c target slightly lower, such as at 7.2%, in order to minimise excessive hyperglycaemia (to reduce the Time Above Range, TAR).
Research finds that 19% of the time the GMI and laboratory HbA1c have an identical value, while 51% of the time they differ by 0.3% (A1c points) or more. It was also highlighted that 28% of the time they differ by 0.5% (A1c points) or more.
Research also shows that the difference between HbA1c and GMI tends to stay consistent for each person over time. If a person has a lower GMI than what their HbA1c suggests (meaning their average glucose is lower than expected), then their GMI is likely to continue to be lower than future HbA1c tests. This may mean that the person has a longer red blood cell lifespan, a higher-than-average glycation rate, or some other biological or genetic factor that isn’t fully understood yet.
Should we use both HbA1c and GMI in diabetes management?
Setting a personal HbA1c target is just one part of an effective glucose management plan. Having access to real-time glucose data and past glucose trends from CGM gives additional information.
Using CGM can help evaluate how well diabetes is being managed, including any time spent in-, above-, or below the target range, and the glucose variability (how much the glucose levels change). In particular Time Below Range and glycaemic variability help to identify any safety concerns that need to be addressed.
For example, a person with a HbA1c of 6.8% who spends 10% of the day in hypoglycaemia needs a different care plan than someone with the same HbA1c who is less than 1% of the day low.
GMI can help both patients and providers see how A1C levels are changing over a shorter time. For instance, if someone starts a new treatment and their GMI drops from 8.5% to 7.8% in two to four weeks, without a significant increase in low blood glucose, it’s likely that the treatment is effective.
What does all this mean in layman’s terms?
To clarify what GMI means to a person with diabetes, it is easiest to explain that GMI is calculated from average CGM glucose readings. It gives an approximate HbA1c level, based on the average glucose level from CGM readings, over 14 or more days.
However, you will also have to explain that the actual laboratory HbA1c may be higher than, or lower, than the GMI because CGMs measure glucose in the interstitial fluid (under the skin), rather than the lab HbA1c results which measure how much glucose has attached to the haemoglobin in the red blood cells. There may be differences in how the glucose attaches to an individual’s red blood cells and there are certain medical conditions that affect the lifespan of a red blood cell. A difference between a laboratory measured A1C and a GMI level, while not unexpected, may be important to consider when evaluating diabetes management.
References:
- Bergenstal RM, Beck RW, Close KL, Grunberger G, Sacks DB, Kowalski A, Brown AS, Heinemann L, Aleppo G, Ryan DB, Riddlesworth TD, Cefalu WT. Glucose Management Indicator (GMI): A New Term for Estimating A1C From Continuous Glucose Monitoring. Diabetes Care. 2018 Nov;41(11):2275-2280. doi: 10.2337/dc18-1581. Epub 2018 Sep 17. PMID: 30224348; PMCID: PMC6196826. https://pmc.ncbi.nlm.nih.gov/articles/PMC6196826/