
5 Expert Tips on Injecting Insulin

Tip #2: Use a recommended injection site
The recommended sites for injections sites are the abdomen, thighs and buttocks3,4. When injecting into the abdomen we should observe the following boundaries:
- At least 1cm above the pubic bones
- A minimum of 1cm below the lowest rib
- At least 1cm away from your navel and
- On the sides, at the flanks (between the ribs and the hip)
Injecting into the arms or legs increases the risk of injecting intramuscularly and therefore should not be done. It can also speed up insulin action when the person exercises. The increased use of the muscles during physical activity can increase glucose absorption due to improved insulin sensitivity, and this can increase the risk of hypoglycaemia3.
Do not use an injection site more than once every 4 weeks.
Tip #3: Use a new needle for every injection
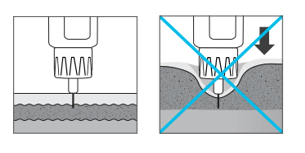
Once, twice, sixteen times… what’s the limit? In actual fact, needles start to become blunt after just one use, it is Best Practice to use a new needle for every injection9.

The image above highlights what happens to the needle, and in particular the needle tip, on multiple uses.
Blunt needles cause increased pain when injecting, as well as more bruising and bleeding. Additionally, there is also an increased risk of skin trauma and infection. This is because the needle loses lubrication and sterilisation after the first use.
Injecting through clothing blunts needles more and can increase the risk of insulin not being injected into the subcutaneous tissue. Particularly if the item of clothing is thick, like jeans, there the recommendation is not to inject through clothes9.
Around 70% of people who reuse pen needles have lipohypertrophy which can increase insulin variability, leading to erratic blood glucose levels.
Tip #4 Reduce the risk of developing lipohypertrophy
Lipohypertrophy, sometimes called a lipo for short, is a thickened “rubbery” swelling of tissue that is sometimes soft and sometimes firm5. The fatty lumps below the skin grow larger over time. Lipohypertrophy causes glucose variability and increases the risk of hypoglycaemia3,6,7.
Although most often you see a raised area, it isn’t always easy to see areas of lipohypertrophy. In many cases it may be easier to feel it.
Lipohypertrophy is the most common complication of insulin treatment and is more common in those with type 1 diabetes than in people with type 2 diabetes. For starters due to the fact that people with type 1 diabetes tend to have a higher number of daily injections but also because people with type 1 diabetes are often injecting for many more years.
Development of lipohypertrophy
There are several factors at play in the development of lipohypertrophy6,8:
- Recurrent injections into the same area Due to repeated trauma to the site, when you do not rotate your injection sites
- The repeated use of the same needle Due to damage to the needle and due to the loss of the lubricant that helps the needle slide through the skin easier
- The use of long (>6mm) pen needles As longer needles cause more discomfort the person may start favouring spots where the discomfort is less, which will lead to overuse of the area
- The insulin itself due to its strong growth-promoting properties
Research has shown that injecting into a lipo can affect blood glucose levels. Such that 39% of people with lipohypertrophy have unexplained hypoglycaemia5.
On average, a person with a lipo can require around 10 units of insulin more every day, compared to people without. This is because the absorption of insulin is not as good. This increased need for insulin can lead to weight gain, which can cause or increase insulin resistance. Interestingly, people with insulin resistance tend to require larger amounts of insulin and as a result can gain further weight and are at increased risk of hypoglycaemia.
If the person switches injections from an area of lipohypertrophy to normal healthy tissue, often a decrease in the insulin dosage is required. This is because the full dose of insulin will be absorbed5. The amount of change varies from one individual to another and should be guided by frequent blood glucose monitoring.
Research has also shown that 99% of those with lipohypertrophy do not rotate their injection sites or don’t rotate correctly5.
Tip #5 Rotate the injection sites
Patients should rotate their injection sites, as not doing this (correctly) and injecting into the same site repeatedly causes lipos to develop.
It is important to move injections at least half an inch (around 1cm or approximately the width of an adult finger) away from the previous injection and to systematically rotate the sites1.
Dividing the injection area into quadrants, using 1 quadrant per week and rotating quadrant to quadrant in a consistent direction, such as clockwise has been proven to reduce the risk of lipohypertrophy and glucose variability. An injection site rotation grid can also be helpful.

Additional tips to reducing pain when injecting insulin
If patients find the injections painful you can recommend the following3:
- Injecting insulin at room temperature rather than when cold.
- If using alcohol to clean the skin (although this is generally not necessary), injecting only after this has dried.
- Using a new needle for each injection.
- Using needles of shorter length and smaller diameter.
- Penetrating the skin quickly with the needle.
- Injecting the insulin slowly.
- Not changing the direction of the needle during insertion and withdrawal.
Other important factors when injecting insulin
It is important to resuspend cloudy insulin before each injection to reduce the risk of hypoglycaemia and glucose variability. The recommended method is gentle mixing by tipping (rocking) and rolling the insulin 10-20 times until the mixture is even in colour without any visible particles. Avoid vigorously shaking the preparation because it can affect the kinetics of the preparation.
Volume of medicine – Insulin absorption is slower with larger doses of insulin and there may be more discomfort and leaking. There is currently no consensus amongst healthcare professionals regarding the largest volume of medicine that can be injected subcutaneously in a single injection. However, for doses over 50 units it is recommended to divide it into 2 injections of smaller doses.
Leakage – Leakage is more related to dose volume and not needle length. If the needle is withdrawn too soon leakage is more likely to occur. To avoid this, increase the time the needle is left in place after the injection.
Air shot – before dialling up a dose, the recommendation is to expel 1-2 units of insulin. Some people try and take a short cut by dialling up a couple of extra units and squirting a bit out before inserting the needle, but this is dangerous as they will squirt out slightly different amounts each time and this could cause dose variability which can affect blood glucose levels.
Preparation of injection site – If the site requires cleaning, soap and water is enough. Alcohol swabs are usually not needed in the home environment and may toughen the skin.
Disposal of sharps – Syringes, pen needles, lancet (finger prickers) and insertion needles for CGM or pump infusion sets are community sharps. Use a puncture-resistant plastic container for disposal. The local hospital, participating pharmacies or at a local community sharps disposal are places to dispose of full sharps containers. Do not dispose of sharps in rubbish bins.
Want to develop your diabetes knowledge further?
References
- Frid AH, Kreugel G, Grassi G et al. Mayo Clin Proc. September 2016:91(9):1232-1233.
- Gibney M, Arce C, Byron K, Hirsch L. Curr Med Res Opin. 2010; 26(6): 1519-1530.
- Australian Diabetes Educators Association (ADEA). Clinical Guiding Principles for Subcutaneous Injection Technique, December 2019.
- Frid AH, Kreugel G, Grassi G et al. Mayo Clin Proc. September 2016:91(9):1231-1255
- Blanco M, Hernandez M, Strauss K, Amaya M et al. Diabetes Metab. 2013; 39(5): 445-53.
- Frid AH, Hirsch LJ, Menchior AR et al. Mayo Clin Proc. September 2016:91(9):1224-1230.
- Vaag A, Damgaard Pedersen K, Lauritzen M, Hildebrandt P, Beck-Nielsen H. Diabetic Medicine 1990; 7: 335-342.
- Look D, Strauss K. Diabetes J. 1998; 10:31-34.
- Fleming Dr, Jacober Sj, Vandenberg Ma, Et AL. The safety of injecting insulin through clothing. Diabetes Care 1997 Mar; 20: 244–7.